Part 1, Strategy 2
Action Item 3: Increase the effectiveness of treatment and support services to improve public safety and health outcomes.
Why it matters
Providing people with the right combination of services isn’t enough to improve public safety or health outcomes. The services delivered must be high quality, research-based, and tailored to the unique needs of people in the criminal justice system. Far too often, behavioral health care providers do not have the necessary specialized knowledge and training on evidence-based practices to provide effective treatment to people in the criminal justice system. A further complication is that existing health care reimbursement rates may not adequately compensate treatment providers for the higher costs often associated with providing effective services for people in the criminal justice system, often resulting in providers who are unwilling or unable to work with this population.
Given the limited availability of effective treatment and services, some criminal justice agencies have created community-based treatment resources exclusively available for people in the criminal justice system. While this strategy can ensure that treatment resources exist to meet the needs of people in the criminal justice system, it doesn’t necessarily improve outcomes or ensure that their treatment needs are met once they leave the criminal justice system.
Instead, policymakers should improve the quality of treatment by ensuring that behavioral health care providers have the training they need on evidence-based practices to advance recovery and reduce recidivism, payment strategies to encourage providing treatment and services to people in the criminal justice system, the means to collaborate with criminal justice and social service agencies, and quality assurance processes to ensure best results. Further, supervision agencies need to be held accountable for reducing recidivism and advancing recovery for people who have behavioral health needs.
What it looks like
- Provide funding and establish standards for quality training for law enforcement staff, court officials, jail, prison, and supervision staff to apply the research on “what works” to appropriately and effectively respond to people who have behavioral health needs.
- Provide funding and establish behavioral health care standards for people diverted from jail to alternatives to incarceration, people on supervision, and people in prison and jail.
- See Case Study: States establish training standards for treatment providers serving people in the criminal justice system
- Require behavioral health treatment providers to apply evidence-based practices to reduce recidivism and improve recovery.
- Develop payment strategies that incentivize treatment providers to deliver specialized services for the criminal justice population.
- Ensure the availability and improve the quality of treatment when issuing grants or contracting for services by including provisions to:
- Prioritize intensive services for people who have the highest risk of reoffending and greatest behavioral health needs.
- Ensure that services are designed to reduce recidivism, improve health outcomes, and advance recovery.
- Hold treatment providers and criminal justice agencies accountable for meeting criminal justice and behavioral health outcome measures.
- Provide financial incentives to treatment providers that exceed standard outcome measures.
- See Case Study: Pennsylvania uses performance-based contracts to reduce recidivism
- Require quality assurance processes and include observations of program delivery as part of regular evaluations of treatment and services.
- See Case Study: North Carolina revamps treatment funding and delivery
Key questions to guide action
- What standards does your state have for providing behavioral health treatment and services to people in jail or prison, as well as in the community?
- Do current contracts with treatment and service providers include provisions and incentives to tie delivery of services to both criminal justice and behavioral health outcomes?
- Does your state require treatment providers or criminal justice agencies to report regularly on criminal justice and behavioral health outcomes?
- How can your state take steps to finance and incentivize the provision of treatment and services that effectively reduce recidivism and advance recovery for people in the criminal justice system who have behavioral health needs?
Use the information that follows to inform your answers to these questions.
Supervision, treatment, and services need to focus on improving behavioral health outcomes and reducing recidivism.
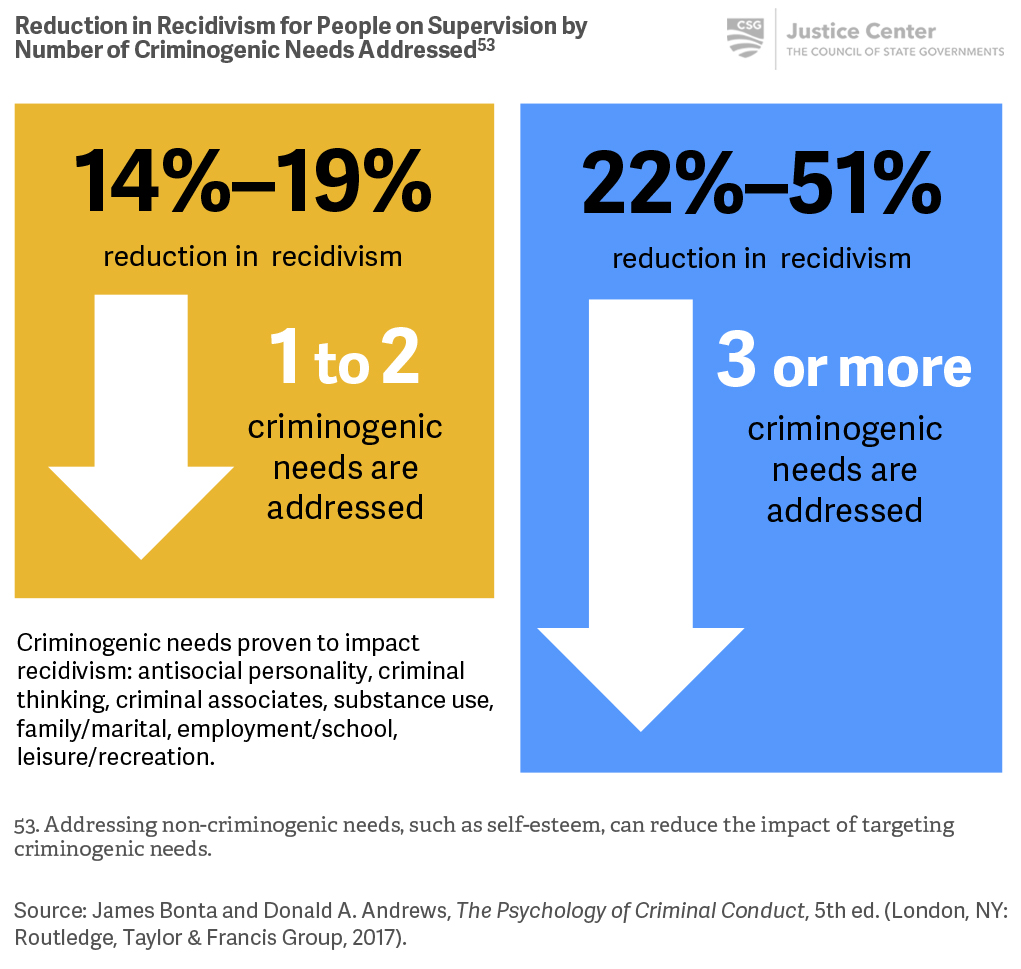
To reduce recidivism among people most likely to reoffend, treatment and services must be coordinated and intensive enough to address their multiple needs.
Case Study
States establish training standards for treatment providers serving people in the criminal justice system
Funding and increasing capacity alone aren’t sufficient to guarantee effective treatment and support services. States also need to ensure that treatment providers are trained to work with people who are on supervision and that they collaborate with supervision agencies to reduce service gaps and enhance coordination.
- West Virginia’s Division of Justice and Community Services requires that community-based treatment providers serving people on supervision complete an eight-class training program covering topics including the use of risk and needs assessment, motivational interviewing, and cognitive behavioral interventions.[49]
- A Kansas law sends people convicted of certain drug offenses to intensive supervision and state-funded certified treatment programs in lieu of correctional facilities. Counselors certified by the Kansas Department of Social and Rehabilitation Services’ Addiction and Prevention Services must complete a four-day training on cognitive-behavioral interventions for people in the criminal justice system to facilitate these treatment programs.[50]
[49] West Virginia Division of Justice and Community Services, Reducing Recidivism and Promoting Recovery West Virginia Implementation Plan for Treatment Supervision (Charleston, WV: West Virginia Division of Justice and Community Services, January 2014).
[50] “Cognitive Behavioral Tools Certification,” Kansas Department of Corrections, https://www.doc.ks.gov/SB123/2003-sb123-training.
Case Study
Pennsylvania uses performance-based contracts to reduce recidivism
After a 2013 internal assessment revealed that people in Community Contract Facilities (CCFs)—halfway houses that help people on parole transition back into society—had higher recidivism rates than people released from prison directly to the community, Pennsylvania’s Department of Corrections (DOC) redesigned its $100 million investment in its community corrections system. The state’s 37 CCFs now provide services such as cognitive behavioral therapy, addiction treatment, and educational/vocational programming, and receive payment based on their ability to reduce recidivism.
If a CCF reduces its recidivism rate below a statewide baseline recidivism range within a given one-year period of the contract, it receives a 1-percent increase in its per client daily charge rate for the next one-year period. Increases in recidivism will result in a warning and possible contract cancellation.
In the first two six-month periods following the change, the DOC found that recidivism declined 11.3 percent overall, 17 CCFs reduced recidivism sufficiently to receive the 1-percent incentive, and 2 received warnings for increased recidivism above the baseline.[51]
[51] Pennsylvania Department of Corrections, “Paying for Success in Community Corrections: Performance Incentive Funding,” (PowerPoint presentation, Statewide Recidivism Reduction Forum, Washington DC, March 8–9, 2016).
Case Study
North Carolina revamps treatment funding and delivery
After North Carolina enacted Justice Reinvestment legislation in 2011, the state eliminated its existing community-based treatment program for people on probation and replaced it with one that evidence shows is more likely to reduce recidivism. Previously, the state funded treatment and services using an outdated grant formula that did not prioritize the state’s limited resources for people who needed them most. As a result, only half of the people who most needed these services received them. In addition, the type and quality of services varied greatly, and there was little impact data being collected, which made it difficult to determine whether these programs were improving outcomes for the people who participated in them.
Today, the state contracts with treatment providers to offer cognitive behavioral interventions and substance addiction treatment to people under supervision, prioritized according to assessed risk and need. When supervision officers identify people on probation who meet the criteria for treatment, they are able to connect them directly to the appropriate services. The state also now requires treatment providers to adhere to stringent quality-assurance standards, collect data, and participate in program evaluations.[52]
[52] CSG Justice Center, “Justice Reinvestment in North Carolina: Three Years Later” (New York: CSG Justice Center, 2014).